This playlist is a collection of all the board review style cases on the site. All the board review style cases on the site in one place! These cases are geared towards preparation for the radiology resident ABR core exam, although similar material is used for the ABR certifying exam general and neuroradiology sections as well as neuroradiology CAQ.
The format of this playlist is case-based. Each case consists of a series of images followed by 1 or 2 questions. The first question is usually to name the diagnosis, while the second is a multiple choice question to test deeper understanding of the specific condition. Try to get the diagnosis before you see the second questions.
Neuroradiology Board Review – Brain Tumors – Case 10
Neuroradiology brain tumor board review. This lecture is geared towards the ABR core exam for residents, but it would be useful for review for the ABR certifying exam or certificate of added qualification (CAQ) exam for neuroradiology.
More description and the answer (spoiler!) are seen below the video.
This case shows you a posterior fossa mass in a child. It his relatively homogeneously T2 hyperintense with relatively avid central enhancement on post-contrast imaging. On ADC, it is relatively dark centrally. A sagittal FLAIR image looks like it confirms that the mass is arising from the cerebellar wall of the ventricle and is displacing the ventricle anteriorly.
Anytime you have a posterior fossa mass in a child, you should be able to list a differential diagnosis, which includes:
pilocytic astroctyoma
ependymoma
medulloblastoma
atypical teratoid/rhabdoid tumor (ATRT)
These are listed in order of decreasing ADC values, because the tumors at the bottom are more cellular and have more tightly packed cells that will be bright on DWI and dark on ADC.
The diagnosis is: medulloblastoma
Medulloblastomas are aggressive tumors in children most commonly found in the posterior fossa. They can be differentiated from other tumors in these age groups by their aggressive appearance and lower ADC values. They arise from the walls of the 4th ventricle or cerebellar hemispheres. There are 4 types (WNT, SHH, group 3, and group 4), but for most radiologists this is beyond the expected knowledge. Genetic features will ultimately guide the prognosis and treatment.
The main differential diagnosis in a child with a lesion such as this is ATRT. I recommend an age based approach to making your differential diagnosis. Because ATRT patients usually are around 6 months old, if a patient is less than 2 years old, choose ATRT. If older, choose medulloblastoma. This will not always be true but is probably true > 95% of the time.
Neuroradiology Board Review – Brain Tumors – Case 9
Neuroradiology brain tumor board review. This lecture is geared towards the ABR core exam for residents, but it would be useful for review for the ABR certifying exam or certificate of added qualification (CAQ) exam for neuroradiology.
More description and the answer (spoiler!) are seen below the video.
This case shows you some images from an axial head CT demonstrating a mass in the lateral ventricles near the septum pellucidum. On CT, it is somewhat heterogeneous. The MRI also shows a heterogeneous mass along the septum pellucidum which has some areas of avid enhancement and some areas of non-enhancement.
Anytime you have an intraventricular mass, you should be able to list a differential diagnosis, which includes:
Meningioma
Central neurocytoma (classic location along septum pellucidum)
Subependymal giant cell tumor (associated with tuberous sclerosis)
Ependymoma
Subependymoma (usually doesn’t enhance)
Choroid plexus tumors (both benign and malignant)
Then, the imaging features can help you favor one diagnosis over the other.
The diagnosis is: central neurocytoma
Central neurocytomas are classically masses along the anterior septum pellucidum near the foramen of Monro. They often look rather heterogenous both on T1, T2, and post-contrast T1. If you see a heterogeneous mass in the lateral ventricle in a testing scenario, it’s probably a central neurocytoma. The other lesions are possible and if you see any of the classical features of other lesions (such as a homogeneous and avidly enhancing mass that looks like a meningioma), you can consider other things.
This patient had a history of melanoma, but you can be pretty confident that this is not a melanoma metastasis because it lacks edema, has heterogeneous non-enhancing components, and has a classic appearance for central neurocytoma. They decided to manage this conservatively with imaging follow-up and it did not change with time, further corroborating the diagnosis.
Neuroradiology Board Review – Brain Tumors – Case 8
Neuroradiology brain tumor board review. This lecture is geared towards the ABR core exam for residents, but it would be useful for review for the ABR certifying exam or certificate of added qualification (CAQ) exam for neuroradiology.
More description and the answer (spoiler!) are seen below the video.
In this case, there is an MRI of the brain in a patient with headache. There is a lesion along the left carotid terminus adjacent to the sella. Its most distinguishing characteristic is that it has intrinsic T1 hyperintensity, is bright on T2/FLAIR, and has relatively no enhancement. There is no associated diffusion abnormality.
One key thing that you need to know to get this case correct is what kinds of things can be intrinsically hyperintense. Blood can be hyperintense at appropriate times (because of methemoglobin). Fat is intrinsically hyperintense. Paramagnetic materials such as gadolinium and manganese are T1 hyperintense. Melanin can also be hyperintense. Because of this relatively short number of things that is intrinsically bright on T1, when you see something that is T1 hyperintense it often has a relatively short differential.
On the CT images, you can confirm that the reason that it is T1 hyperintense is because the lesion contains fat. Additionally, you can see additional unexpected areas of fat in the sylvian fissure and quadrigeminal plate cistern.
The diagnosis is: ruptured dermoid
Dermoids are part of the spectrum of masses from retained embryonal tissues, with the other possibilities including epidermoid and teratoma. The major characteristic of dermoids is they have internal fat contents and are not bright on DWI. These can rupture and cause a chemical meningitis from irritation of fat in the subarachnoid space. This can lead to a number of symptoms such as headache or seizure. Dermoids are often resected but they are indolent lesions which are non-aggressive.
Neuroradiology Board Review – Brain Tumors – Case 7
Neuroradiology brain tumor board review. This lecture is geared towards the ABR core exam for residents, but it would be useful for review for the ABR certifying exam or certificate of added qualification (CAQ) exam for neuroradiology.
More description and the answer (spoiler!) are seen below the video.
The CT of the head shows a lesion in the right temporal lobe with masslike expansion and calcification.
0:55 The differential diagnosis for calcified lesions in the brain is pretty selective. A few tumors, including oligodendroglioma, meningioma, and pleomorphic xanthoastrocytoma (PXA) are well known for calcification. Only a few metastases calcify, and those are mostly bone tumors like osteosarcoma and chondrosarcoma. Vascular lesions including arteriovenous malformations (AVM) and cavernous malformations can also calcify, but the calcifications may look vascular.
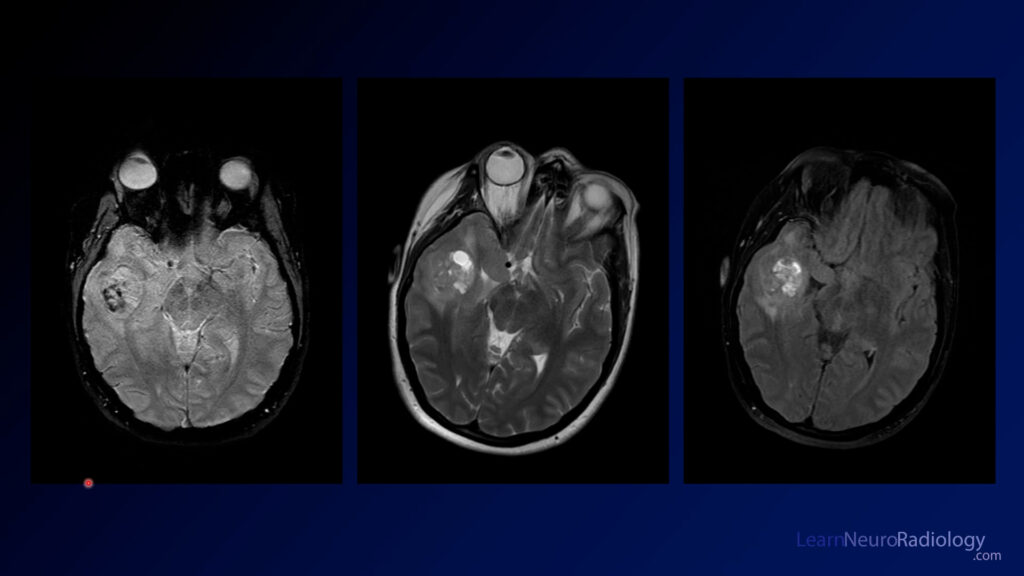
The MRI shows a heterogeneous mass in the right temporal lobe. There are T2 hyperintense areas of non-enhancement that appear almost cystic. There is some surrounding edema, although the extent of mass effect is less than expected given the size of the mass. GRE or susceptibility imaging show areas of hypointensity likely corresponding to the calcification on CT. On post-contrast imaging, there is heterogeneous, irregular enhancement with a broad dural margin.
2:12 The diagnosis is: pleomorphic xanthoastrocytoma (PXA)
PXAs are relatively rare tumors occurring in teenagers and younger adults. They are WHO grade 2 tumors. They are most commonly supratentorial. A classic trademark is a dural tail, which is relatively uncommon for intraparenchymal tumors. In many cases they can look like a much more aggressive tumor, but it is a nice clue if it has less mass effect than expected. Think about PXA if you see a tumor that looks more aggressive than it should for size and mass effect.
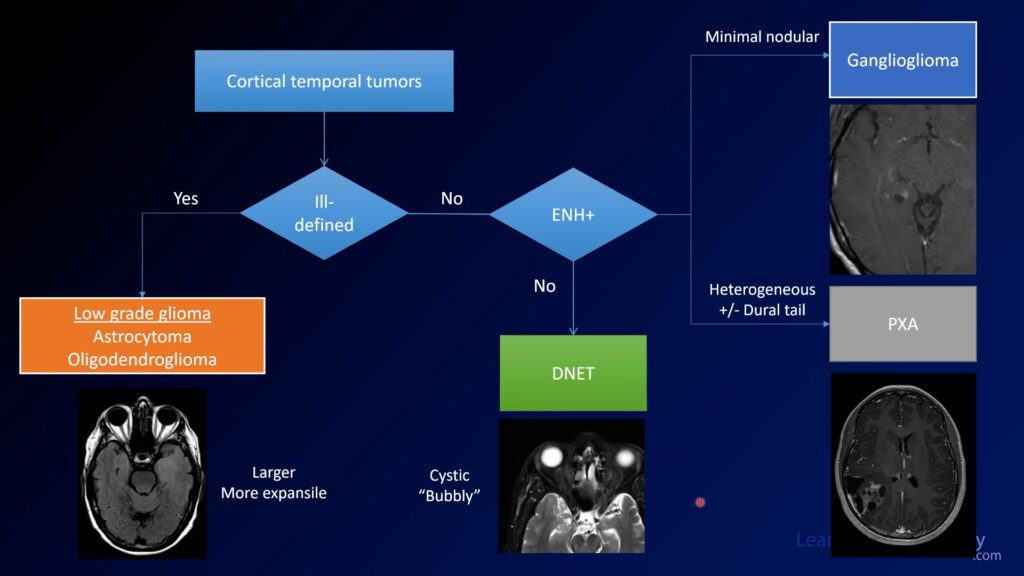
Framework for evaluating cortical temporal tumors. There are a few common tumors you may encounter in the temporal lobes in seizure patients. First consider whether they are ill-defined or well-marginated. If ill-defined, the differential includes astrocytoma or oligodendroglioma. If well-marginated, then consider whether there is enhancement. If no enhancement, DNET is most likely. If there is a small amount of nodular enhancement, favor ganglioglioma. As in this case, PXAs tend to have more enhancement in a more irregular pattern.
In summary, it is helpful to have an approach to cortical tumors that can help you differentiate these lesions. Remember, it can be challenging to differentiate them without a biopsy in real life, but it is nice to be able to hone your differential diagnosis.
Neuroradiology Board Review – Brain Tumors – Case 6
Neuroradiology brain tumor board review. This lecture is geared towards the ABR core exam for residents, but it would be useful for review for the ABR certifying exam or certificate of added qualification (CAQ) exam for neuroradiology.
More description and the answer (spoiler!) are seen below the video.
This case shows images from an MRI of the posterior fossa. There is a mass in the right cerebellar hemisphere that has a predominantly cystic component and an enhancing nodule along the margin. There is some mass effect with effacement of the fourth ventricle.
The differential diagnosis for a posterior fossa cyst with a nodule has two main entities: pilocytic astrocytoma and hemangioblastoma. Pilocytic astrocytomas are the most common in children and young adults while hemangioblastomas are more common in adults. If you see flow voids on T2, that is also a nice clue that you are looking at a hemangioblastoma.
The diagnosis is: hemangioblastoma
Hemangioblastomas are cystic and solid masses that are commonly seen in the posterior fossa and spine. While they are often associated with von Hippel Lindau syndrome, the vast majority are sporadic (75-80%). They are usually cystic lesions with a solid nodule and minimal wall enhancement. Surgery can be curative, particularly if the entire enhancing nodule is resected, but it is not sufficient to drain the cystic component.
von Hippel Lindau is a syndrome of multiple lesions, with the most common in the kidneys (RCC, renal cysts, and angiomyolipomas). They are also associated with pancreatic cysts, adrenal pheochromocytomas, and other lesions. Think about this any time you see a CNS lesion with a corresponding abnormality elsewhere in the body.
Neuroradiology Board Review – Brain Tumors – Case 5
Neuroradiology brain tumor board review. This lecture is geared towards the ABR core exam for residents, but it would be useful for review for the ABR certifying exam or certificate of added qualification (CAQ) exam for neuroradiology.
More description and the answer (spoiler!) are seen below the video.
This case shows images from an MRI through the sella, including both coronal and sagittal images. There is expansion of the sella with a T1 isointense, T2 hyperintense mass replacing the sella and extending beyond the margins of the sella, including the cavernous sinuses bilaterally. The sella itself is also expanded. On postcontrast imaging, you see a pretty avidly enhancing sellar and suprasellar mass with no real risidual pituitary seen.
The diagnosis is: pituitary adenoma
Pituitary adenomas are extremely common brain masses and are very common incidental masses. They arise in the sella but can extend into the cavernous sinuses and suprasellar region. About half of these masses are non-secreting, while the most common secreting tumor is a prolactinoma. On imaging, they often enhance but typically enhance a little bit less than the surrounding normal pituitary. They can hemorrhage and have cystic degeneration. Because adenomas are slow-growing lesion, the sella is often expanded and remodeled but may not be completely destroyed.
When patients have pituitary hemorrhage, this is called apoplexy. This most often occurs in patients with an underlying adenoma. This is associated with a variety of conditions, including pregnancy/postpartum state, treatment of a prolactinoma with bromocriptine, and cerebral angiography (although admittedly I’ve never seen this).
Neuroradiology Board Review – Brain Tumors – Case 4
Neuroradiology brain tumor board review. This lecture is geared towards the ABR core exam for residents, but it would be useful for review for the ABR certifying exam or certificate of added qualification (CAQ) exam for neuroradiology.
More description and the answer (spoiler!) are seen below the video.
This case shows images from an MRI through the level of the pons. There is a mass in the left cerebellopontine angle (CP angle). It is causing mass effect on the pons. On postcontrast imaging, you can see that it is avidly enhancing with a few central areas of non-enhancement. A key to this case is identifying where the mass is centered. Does it look like it’s outside the IAC or centered in and expanding the IAC?
The diagnosis is: vestibular schwannoma
Vestibular schwannomas are extraaxial masses arising from the vestibular nerve (8th cranial nerve) either as they pass through the cerebellopontine cistern or in the internal auditory canal. They were previously called acoustic neuromas, but it is preferable to call them vestibular schwannomas given our current understanding of them. A key imaging feature is that they expand the internal auditory canal (IAC).
When approaching a cerebellopontine angle mass, it is useful to take a two step approach. First, determine if you think it is mostly solid and has enhancing components. If so, then think about schwannoma or meningioma as your top two differential considerations. If it is centered in the IAC and causes IAC enhancement, it’s probably a schwannoma. Meningiomas in this location occur but are more likely to have only minimal extension into the IAC without expansion.
This patient also had hydrocephalus from compression of the 4th ventricular outflow. Remember that masses in the posterior fossa can cause hydrocephalus due to mass effect.
Neuroradiology Board Review – Brain Tumors – Case 3
Neuroradiology brain tumor board review. This lecture is geared towards the ABR core exam for residents, but it would be useful for review for the ABR certifying exam or certificate of added qualification (CAQ) exam for neuroradiology.
More description and the answer (spoiler!) are seen below the video.
This case shows a single image from a head CT as well as some MRI images at the same level. There is a dominant mass in the left parietal lobe which has some internal blood products. There is surrounding edema, but not much enhancement as most of the T1 hyperintensity is intrinsic (present on the pre-contrast exam) from blood products/methemoglobin. Upon closer inspection, there is also a smaller enhancing nodule in the adjacent cerebral hemisphere.
The diagnosis is: metastatic disease
Metastases to the brain are common manifestations of malignancies elsewhere in the body. The most common diseases to cause brain metastases are the same as the most common systemic cancers, including lung cancer, breast cancer, and melanoma. When brain metastases have hemorrhage, you might think about melanoma, renal cancer, and thyroid cancer (among others).
The most common locations for brain metastases are in the cerebral hemispheres and cerebellum. About 50% of brain metastases are solitary, so don’t be fooled if you see only a single lesion. It can still be a metastasis.
The differential diagnosis for most metastatic lesions includes infection and high grade glioma. Demyelinating disease can also sometimes have a similar appearance.
Neuroradiology Board Review – Brain Tumors – Case 2
Neuroradiology brain tumor board review. This lecture is geared towards the ABR core exam for residents, but it would be useful for review for the ABR certifying exam or certificate of added qualification (CAQ) exam for neuroradiology.
More description and the answer (spoiler!) are seen below the video.
This case shows an MRI of the brain with a pretty well-defined, expansile mass in the inferior aspects of the right parietal lobe with some extension into the adjacent frontal and temporal lobes. It is markedly T2 hyperintense, but somewhat less intense centrally on FLAIR. On pre- and post-contrast imaging, this shows that the tumor is predominantly non-enhancing, although there is a thin rim of enhancement around the anterior margin.
The diagnosis is: anaplastic astrocytoma (grade 3)
Anaplastic astrocytomas are grade 3 astrocytomas that are most commonly IDH mutated. They tend to have slightly more mass effect and enhancement than grade 2 tumors but do not have the necrosis and avid enhancement of grade 4 tumors most of the time. 1p19q codeletion is absent in these tumors because if present these would be oligodendrogliomas.
The T2 mismatch sign is a relatively recently described imaging finding of IDH mutated astrocytomas. When a portion of the tumor is very bright on T2 but suppresses on FLAIR, this is a pretty specific sign for IDH-mutation. This fact could appear on an ABR exam, especially the CAQ exam.