Brain tumors
Brain tumors are one of the most common diagnoses addressed in neuroradiology. This covers a wide spectrum of disease, from primary brain tumors like gliomas and glioblastomas to secondary disease like metastases.
Brain tumors are classified by their histology or cell of origin and genetics. Tumors can be divided into a few categories, including astrocytomas, oligodendrogliomas, other low grade glial tumors, and common non-glial tumors. Since the WHO reclassification occurred in 2016, genetic information has been used to classify tumors, with the most important mutations being isocitrate dehydrogenase (IDH), 1p19q codeletion, and MGMT methylation. Oligodendrogliomas must be IDH mutants and 1p19q codeleted, and other tumors are now classified as astrocytomas.
IDH mutation is associated with lower grade astrocytomas and is associated with a survival advantage. Similar, MGMT methylation is associated with a better response to radiation, more pseudoprogression, and better survival. For more information, check out the video introduction.

Gliomas
Gliomas are tumors which arise from the support cells in the brain, including astrocytes and oligodendrogliocytes. Gliomas are the most common primary parenchymal brain tumor, with the most common being glioblastoma (GBM, grade 4 astrocytoma).
Astrocytomas
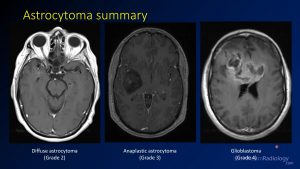
Astrocytomas are the most common glial tumors and include low grade astrocytomas (WHO grade 2), anaplastic astrocytoma (grade 3), and glioblastoma (grade 4). By definition, these tumors have intact 1p19q. They can have either IDH mutation or IDH wild type, and IDH mutation is associated with increased survival. Higher grade tumors are more likely to have more mass effect, more enhancement, and less well-defined margins.
Oligodendrogliomas
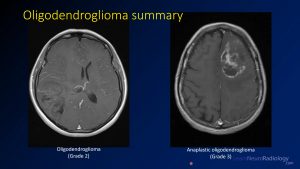
Oligodendrogliomas include low grade oligodendrogliomas (WHO grade 2) and anaplastic oligodendroglioma (grade 3). By definition, these tumors have 1p19q codeletion and IDH mutation. Oligodendrogliomas have better survival than astrocytomas. Higher grade tumors are more likely to have more mass effect, more enhancement, and less well-defined margins. However, oligodendrogliomas typically do not degenerate into glioblastomas.
Other low grade gliomas
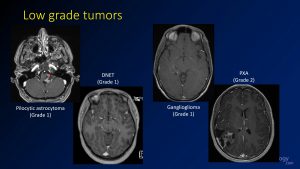
Some less common low grade tumors include pilocytic astrocytoma, dysembryoplastic neuroepithelial tumor (DNET), ganglioglioma, and pleomorphic xanthoastrocytoma (PXA). These tumors are often seen in younger patients, many of whom will present with seizures. Surgery is often curative. There is a lot of imaging overlap for these tumors, especially DNET and ganglioglioma, which can appear very similar. However, the specific diagnosis is less important than knowing that a lesion may be a low grade glioma.
Non glial tumors
There are several common non-glial brain tumors, such as lymphoma, metastasis, and meningioma.
Lymphoma is a common brain tumor which can be either associated with systemic lymphoma or more commonly confined to the brain (primary central nervous system, CNS, lymphoma). It is associated with immunosuppression and HIV. Metastatic disease is also common, and it’s important to remember that up to 50% of intracranial metastases are solitary. Meningiomas are the most common brain tumors overall and are extra-axial lesions. They come in 3 grades, and grade 2 and 3 are often irradiated after resection.
Common imaging scenarios
There are a few common scenarios you may encounter when imaging, such as a solitary enhancing lesion, multiple enhancing lesions, and non-enhancing peripheral lesions. Each of these has a differential diagnosis, and choosing appropriately can help guide therapy.
For example, the differential for a solitary enhancing mass is:
- Glioblastoma
- Metastasis
- Lymphoma
- Abscess (you should be able to rule out or in based on diffusion)
- Infection
Similarly, the differential for a multiple enhancing parenchymal masses is:
- Metastases
- Lymphoma
- Multifocal glioblastoma
- Abscesses (you should be able to rule out or in based on diffusion)
- Infection
The differential diagnosis for a well-defined minimally enhancing cortical tumor is:
The differential diagnosis for a well-defined minimally enhancing cortical tumor is:
- DNET
- Ganglioglioma
- PXA
If cortical tumor is ill-defined, it is probably a low-grade glioma.
Finally, the differential diagnosis for a tumor with a cyst and a nodule is:
- Pilocytic astrocytoma
- Ganglioglioma
- Hemangioblastoma (has blood vessels/flow voids)
- PXA
Practice cases
Bonus cases
To work on your skills in properly identifying and diagnosing brain tumors, check out the
Books/other resources
Many of the resources for learning about brain tumors are pretty advanced. There are sections in several books, including
Brain Tumor Imaging – Rajan Jain & Marco Essig
This is a pretty good book that covers the entire scope of brain tumor imaging pretty well, including the use of advanced imaging such as spectroscopy and perfusion.