Spine tumors
Spine tumors can be a challenging topic for a neuroradiologist because we deal less with tumors in the spinal cord and spinal canal. However, there is a relatively simple approach that can help you hone your differential diagnosis. This involves taking a location-based approach which divides the spinal canal into 3 main regions. This series of videos shows the general approach as well as specifics about making a differential diagnosis in each of these locations.
Location based approach
Spine tumors can be a challenging topic for a neuroradiologist because we deal less with tumors in the spinal cord and spinal canal. However, there is a relatively simple approach that can hep you hone your differential diagnosis. This involves taking a location-based approach which divides the spinal canal into 3 main regions.
- Intramedullary – in the spinal cord
- Extramedullary intradural – in the thecal sac (within the dura) but outside the spinal cord
- Extradural – outside the dura
Then, you can formulate your differential based on the normal structures in those regions. You can’t always tell the exactly location of a lesion, but you can use the displacement of normal structures to help you try to decide. Then you know how to guide your differential.
Intramedullary lesions
The most common intramedullary tumors are primary tumors of the cord itself, most commonly ependymomas and astrocytomas. Other things such as hemangioblastoma and cavernous malformations can also happen in the spinal cord. Check out the lecture about intramedullary lesions to learn more about what types of things should be included in your differential diagnosis.
Intramedullary tumor mimics
There are a wide range of lesions occurring in the spinal cord which can mimic tumors. This includes vascular lesions, inflammatory/demyelinating disease, sarcoid, and CSF flow abnormalities. This video takes a look at some of the range of possibilities.
Extramedullary intradural lesions
Lesions that occur within the thecal sac are categorized as intradural extramedullary lesions. The vast majority of these lesions are tumors. The most common are schwannomas (and other nerve sheath tumors) and meningiomas, but there are others that include ependymoma, metastatic disease, and lymphoma. Also remember that the intradural extramedullary space contains cerebrospinal fluid (CSF), so any process that diffusely affects CSF can affect this space.
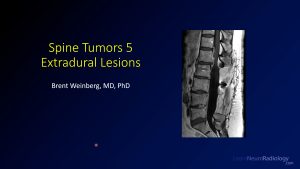
Extradural lesions
Lesions outside the thecal sac are categorized as extradural lesions. Remember that everything that isn’t in the thecal sac is extradural, including discs, bones, meninges, nerves, and blood vessels. Anything that can occur in the surrounding areas can have extradural components. Look for lesions that have mass effect on the dura and deflect both the dura and the thecal sac to the side. Many of these lesions will require a biopsy as they have a differential diagnosis on imaging. CT and diffusion weighted imaging are useful adjunct tools that can help you refine your diagnosis.
Cystic lesions
A few lesions within the spinal canal are predominantly cystic or nonenhancing. They are almost always intradural extramedullary. The three most common entities are arachnoid cysts, dermoid cysts, and neuroenteric cysts. A contrast enhanced myelogram can often give you a little bit more information about what the entity is by determining if it fills with contrast.
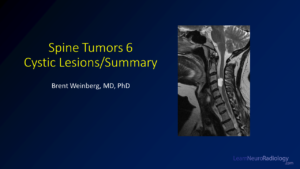
Summary
Overall, when thinking about spine tumor, you should take a location-based approach. When divided by intramedullary, intradural extramedullary, and extradural, this can help you decide what type of lesion you are dealing with. Overall, always remember that the spine is an extension of the central nervous system, and consider imaging the brain because that may help you hone your differential diagnosis.