Neuroradiology Board Review – Brain Tumors – Case 10
Neuroradiology brain tumor board review. This lecture is geared towards the ABR core exam for residents, but it would be useful for review for the ABR certifying exam or certificate of added qualification (CAQ) exam for neuroradiology.
More description and the answer (spoiler!) are seen below the video.
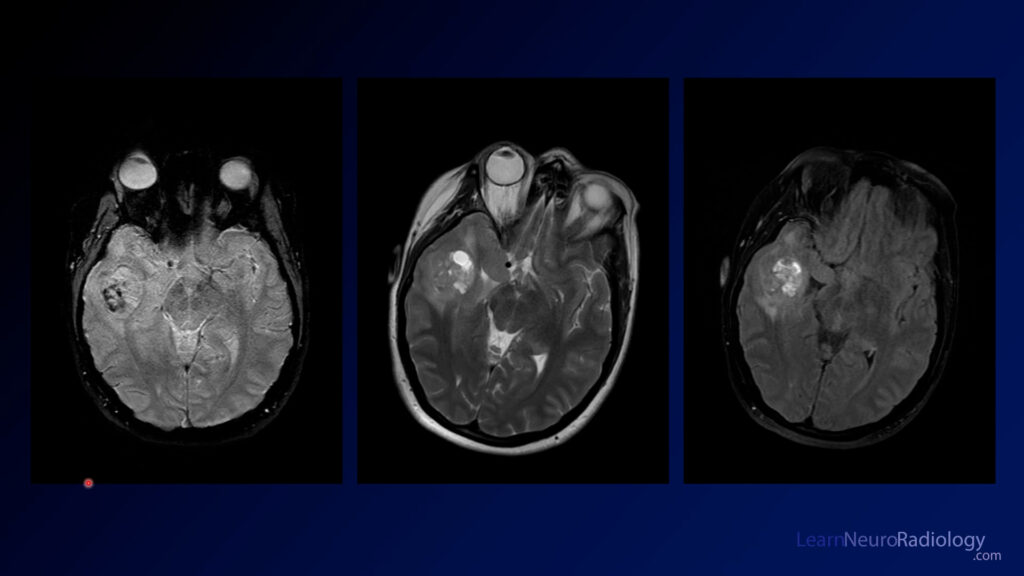
This case shows you a posterior fossa mass in a child. It his relatively homogeneously T2 hyperintense with relatively avid central enhancement on post-contrast imaging. On ADC, it is relatively dark centrally. A sagittal FLAIR image looks like it confirms that the mass is arising from the cerebellar wall of the ventricle and is displacing the ventricle anteriorly.
Anytime you have a posterior fossa mass in a child, you should be able to list a differential diagnosis, which includes:
- pilocytic astroctyoma
- ependymoma
- medulloblastoma
- atypical teratoid/rhabdoid tumor (ATRT)
These are listed in order of decreasing ADC values, because the tumors at the bottom are more cellular and have more tightly packed cells that will be bright on DWI and dark on ADC.
The diagnosis is: medulloblastoma
Medulloblastomas are aggressive tumors in children most commonly found in the posterior fossa. They can be differentiated from other tumors in these age groups by their aggressive appearance and lower ADC values. They arise from the walls of the 4th ventricle or cerebellar hemispheres. There are 4 types (WNT, SHH, group 3, and group 4), but for most radiologists this is beyond the expected knowledge. Genetic features will ultimately guide the prognosis and treatment.
The main differential diagnosis in a child with a lesion such as this is ATRT. I recommend an age based approach to making your differential diagnosis. Because ATRT patients usually are around 6 months old, if a patient is less than 2 years old, choose ATRT. If older, choose medulloblastoma. This will not always be true but is probably true > 95% of the time.